Muhimbili National Hospital, Dar es Salaam, Tanzania: WEO training course August 12–15, 2024
Tanzania is a strategically located country with many of the features we are aiming for in our selection of training centers. The Muhimbili National Hospital (MNH) is by far the biggest hospital in the country, 100% public, and seeming in many respects to outperform the private alternatives.
Initial meeting with MNH CEO - Prof Mohamed Janabi (centre) in 2023 Our main contact, Dr. John Rwegasha, was previously Head of GI, then Head of Internal Medicine, and has recently been promoted to Director of Medical Services. He is an endoscopist and hepatologist, still maintaining his endoscopic duties in addition to his substantial administrative role.
The collaboration between MNH and WEO was established after two previous visits and an MoU was signed in January 2023. This year, a 4-day training course was devised, following discussions with the team.
I was accompanied by Dr. Darshan Parekh from Mumbai, representing our initial expansion of travelling faculty following the website recruitment along with personal communications. Dr Parekh is a highly skilled advanced endoscopist, providing substantial important input in addition to his teaching talents.
Initial meeting with MNH CEO - Prof Mohamed Janabi (centre) in 2023
The hospital is by far the biggest public hospital and educational unit in Tanzania. The endoscopy department remains impeccably equipped with three examination rooms having Olympus equipment, including two Exera III and one X1 tower, eight gastroscopes, three colonoscopes, and two duodenoscopes, plus a Fujifilm EUS tower and a linear EUS endoscope. All endoscopes appear operational. The unit is operated by surgeons (two days), and gastroenterologists (two days) with one day for bronchoscopy, but there is some overlap.
Unfortunately, the C-arm was awaiting repair (along with two other broken C-arms in the Biomed Tech office).
Wifi is still not accessible in the endoscopy unit; the 4G signal is quite unstable and weak in most rooms. There are no explicit plans for improvement of this. However, the unit has a dedicated medtech member of staff who is very committed and who would look into it.
The training course was structured similarly to previous courses, with three-and-a-half days of activities adapted to maximize hands-on exposure. It was not easy to recruit external participants unfortunately, but we had training with three medical and three surgical faculty plus a total of five fellows from both departments. In addition, nurses participated, as well as some on-site reps from China who brought an Aouha demonstration endoscopy tower and endoscopes; they also joined some of the lectures.
Didactic talks included basic endoscope structure, error-solving and maintenance, basic colonoscopy techniques, detection, assessment and removal of polyps, and basic ERCP cannulation techniques. Generally there were 10–12 people in the room including some of the nurses.
Hands-on training generally comprised 15–20 cases per day, with two thirds being EGDs.
For colonoscopy, the quality of colon cleansing quality was moderate, but the cecal intubation rate was quite good. There were several cases of colorectal cancer, including in young people, one case of colitis, and very few polyps. Polyps >10 mm were generally left for subsequent surgery(!). Cold snaring was not utlized.
Regarding EGD, a number of moderate esophageal varices were banded with reasonable technique. There was one case with weblike strictures above the varices that required bougienage in order to pass the band ligator. Placement of an esophageal stent without fluoroscopy in a case of distal esophageal cancer worked flawlessly. Another patient had proximal squamous cell cancer.
On Monday afternoon we had a very useful multidisciplinary meeting with GI, surgeons, and an oncologist, discussing a number of hepatobiliary cases where ERCP and EUS might be relevant. The meeting room allowed for a display of all available imaging, and the discussions were lively and very productive, resulting in real benefits for the patients discussed.
Documentation is template-based and available in the hospital system but without database options.
Dr. Darshan discussing a case with Dr. Justine
We carried out one ERCP without a C-arm, in a patient with a distal stone, aspirating bile for verification of cannulation before sphincterotomy and balloon sweeping. We also performed four EUS procedures, in two cases for distal esophageal lesions that were not present. Cases were also used to demonstrate standard anatomy. Most routine procedures were done by local faculty or by fellows with faculty support. We intervened very little, except for the ERCP and EUS procedures.
Band ligation of large esophageal varices
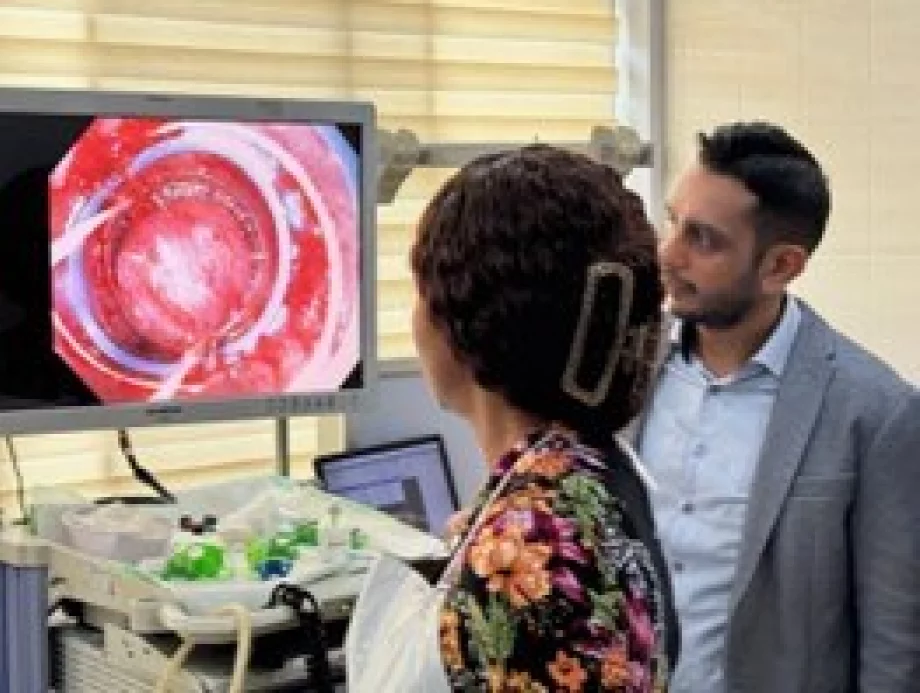
First EUS case at MNH
Equipment. The towers and endoscopes were excellent, including a trial system from Aouha, which was a high-end tower with advanced AI support. Band ligators from China were also available. As previously reported, an in-house pharmacy offers accessories for purchase by patients prior to planned procedures, but with a small emergency selection of equipment for special needs.
MicroTech kindly offered a selection of material for the course; this was a great support and, for them, also excellent exposure of their quality material. Manual scope reprocessing facilities were spacious, clean, and user-friendly, including covered storage for the majority of scopes.
Telementoring potential. We wanted to explore telementoring as part of continuous center support. Wifi was not available but there was cabled internet in all examination rooms. The extremely helpful biotech member of staff and Charles from IT helped with necessary installations (Zoom and video OBS [Open BroadcasterSoftware]) on the standard desktop computer. With this and some appropriate cables and converters we did a live transmission of the ERCP procedure to Oslo and Canberra with quite acceptable video and sound quality. This will be explored further but this setup eliminates the need for wifi routers which are notoriously difficult to obtain.
Transmitted video of ERCP procedure recorded in Oslo Norway
Meeting with department leadership, Dr. Rwegasha to the right
Meetings. We had a startup meeting with John Rwegasha about the plans for the course and also for future collaboration. We also met with the MNH CEO, Professor Mohammed Janabi, who offered strong support for continued collaboration. On the last evening we had a pleasant dinner meeting with John, Eva (head of GI), and the head of the medical department to discuss next steps. This will include repeat visits, but also a plan for two faculty to go to India for high volume training in ERCP and EUS, provided there is available equipment in the unit. We discussed how to optimize the output from faculty visits such as the present one, including planning modifications of the program, lineup of useful teaching cases etc.
Altogether a very helpful visit, for us and hopefully also for the unit at Muhimbili National Hospital. We will be back!