Most colorectal polyps are <10 mm in size, and easy to resect using standard polypectomy techniques. However, endoscopists may encounter large, flat, or sessile and ≥20 mm laterally spreading lesions (LSLs) which require special techniques and expertise for effective and safe resection. The technique of choice for most large LSLs is endoscopic mucosal resection (EMR), which has been shown to be more cost-effective and safer than surgical resection. These types of procedures take longer than routine ones and require additional training and experience to master. Below are principles, tips, and tricks that can help ensure successful resection and optimize outcomes.
- The first and critical step in EMR of LSLs is determining which lesions should not be resected endoscopically, and should instead be referred to surgery because of features suggestive of deep invasion. This requires detailed lesion assessment, and facility with classification and characterization schemes, including the Japanese-Paris classification, Kudo pit patterns, and topography (granular or non-granular surface).
- The goal of EMR is to complete the procedure in the first session. Every endoscopist with EMR expertise will tell you that lesions which have been previously manipulated or partially resected can be very challenging to treat because of submucosal fibrosis. The other issue to consider is the presence of appropriate support (trained and experienced technician, surgical backup). Never start unless you are certain that you can finish! If you are uncertain, consider referring the patient to a tertiary facility that has the required expertise.
- Decide on the resection strategy before you begin and anticipate what you want in your toolbox, so your technician is prepared and the resection can proceed efficiently. This includes type(s) of snares, electrocautery settings, hemostatic clip placement, and tattooing.
- Submucosal injection should be considered for all large LSLs, and should include a contrast agent (indigocarmine or methylene blue) to delineate the resection plane and lesion border. Normal saline is an adequate and cheap submucosal injectate, but it is not durable and may entail repeated injections. Newer proprietary preparations include both fluid and dye and last longer, thus reducing EMR time, but are more expensive.
- Start injecting just before puncturing the mucosa, as this will help find the submucosal plane quickly. It is appropriate to inject the lesion itself or its border, but never an ulcerated or depressed area. Always watch for areas that do not lift adequately, as this may indicate fibrosis or invasion.
- Resection should aim for as few pieces as possible, but individual piece size should not exceed 20mm each, to minimize risk of deep thermal injury. Use a 15-mm or 20-mm stiff snare for the initial bulky resections, and a microprocessor-controlled primarily “cutting” current. Aim to include 2–3 mm of normal tissue rim, and with each resection pass use the defect created by the previous resection to anchor the snare.
- If there are residual islands, use a small stiff snare or hot avulsion forceps to complete resection. Do not use ablative modalities such as argon plasma coagulation. After completion of EMR, treat the edges (even if normal-appearing) using snare-tip soft coagulation (STSC).
- Place hemostatic clips if possible, particularly for LSLs in the right colon or if the patient is on anticoagulants. Aim for complete closure of the defect if this is feasible.
- Mark all LSL resection sites by tattooing, with the possible exception of cecal lesion sites. Always avoid injecting the resection site itself, and target 2–3cm distally. The needle should be directed tangentially to the mucosa, not perpendicularly. Describe the location of the tattoos in the endoscopy report, and include photodocumentation showing the tattoos in relation to the resection site, to facilitate subsequent locating.
- Bring the patient back for surveillance in 3 to 6 months. Ensure that the requirement for early surveillance is clear from the outset (i.e., discussed during the initial informed consent process), because most residual/recurrent neoplasia will be detected at that first follow-up, and a negative examination is highly predictive of long-term success.
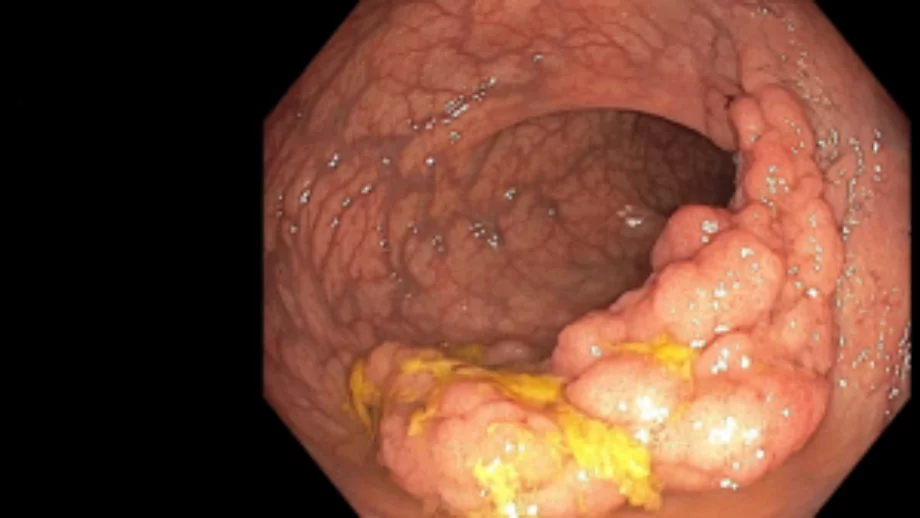
Large rectal LSL, type IS/IIA-G
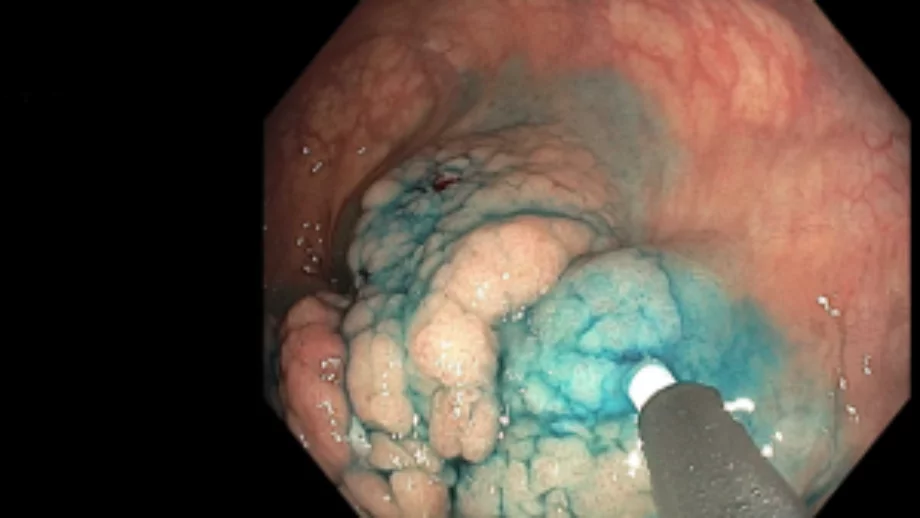
Dynamic submucosal injection, with adequate lift
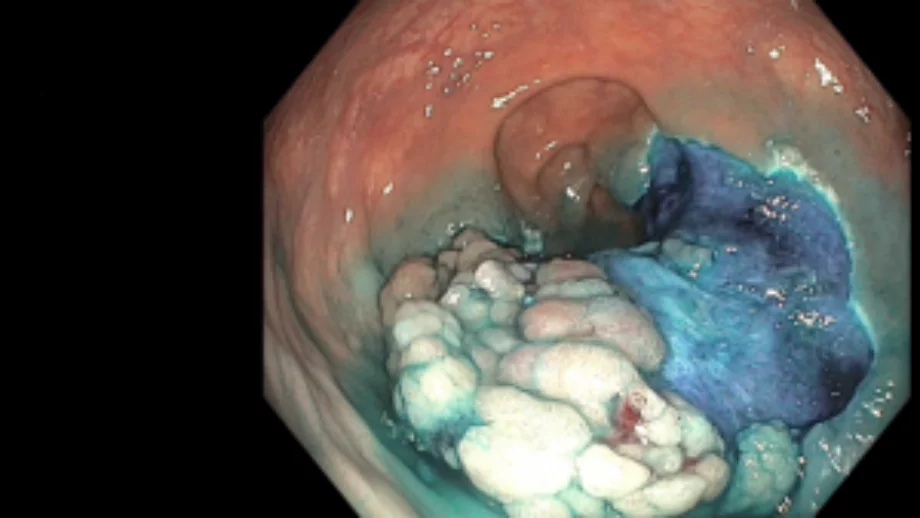
Piecemeal resection
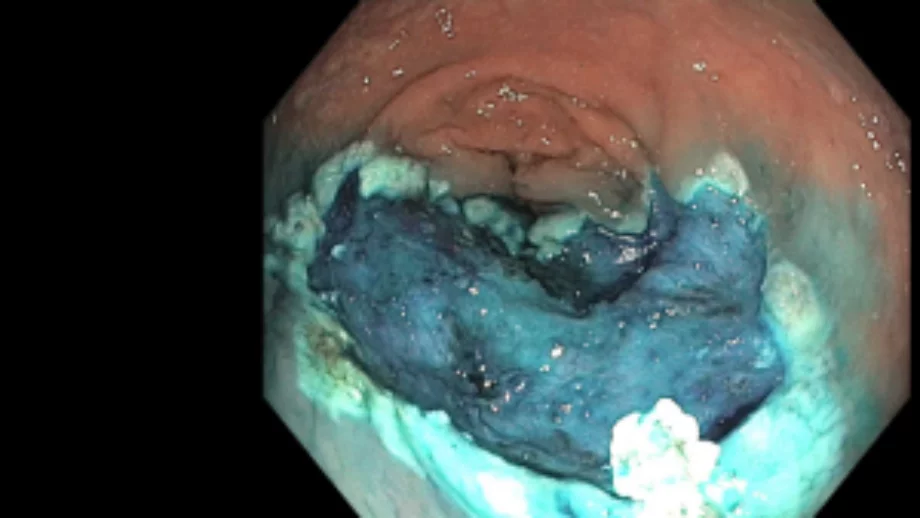
Resection defect, with edges treated with STSC
About the Author
Dr Charles Kahi
Gastroenterologist and Professor of Clinical Medicine at Indiana University School of Medicine in Indianapolis, Indiana, USA